
Since the advent of injectable dermal fillers, the quest for the perfect filler has been a lofty goal. The perfect filler would integrate smoothly into tissue, cause minimal oedema and inflammation, be easily reversible, be devoid of any type of foreign body response, be non-allergenic, be stable and predictable, breaking down into to nonimmunogenic particles and be naturally absorbed or dissolved without incident. Unfortunately, such a filler does not exist. Since the Food and Drug Administration’s (FDA) approval of injectable bovine collagen in the early 1980s, dozens of injectable filling agents have been developed; but history has taught us that new technologies must be used with care because complications can occur, sometimes many years after treatment (Kontis and Rivkin, 2009).
Dermal fillers are no exception. While the vast majority of patients have good outcomes, late onset adverse reactions have been reported with all the available products on the market.
It is commonly accepted that the inflammatory cascade and subsequent healing process are responsible for the results of many cosmetic interventions, including energy-based therapies, platelet rich plasma and even injectable fillers. The creation of multiple micro injuries initiates the healing response, and the body is left to repair itself. This healing process is fascinating, complex, and still not completely elucidated. It encompasses two separate processes: regeneration and replacement (Krafts, 2010). Regeneration refers to a type of healing in which new growth completely restores portions of damaged tissue to their normal state, whereas replacement refers to healing of severely damaged tissues by laying down connective tissue, commonly called scarring (Krafts, 2010), with less function or nonfunction of the new tissue. The goal of regenerative medicine is to provide a substitute for tissues lost to trauma, disease, congenital abnormalities (Chung et al, 2017) and to restore tissue function back to physiological activity (Griffin et al, 2021). In the case of aesthetic regenerative medicine, the goal is to revive aging tissue, especially the skin, and return to it physiologic activities such as hair growth and collagen and elastin generation.
In normal wound healing, most of the time, a combination of replacement and regeneration occurs. In developing fetal skin, wounds are capable of healing completely by regeneration, which results in scar free healing (Wilgus, 2020). Certain animals, such as an amphibian, the axolotl, can achieve ‘perfect, scar free skin regeneration’, after full thickness skin excision and are even able to regenerate complete organs (Reinke and Sorg, 2012). In contrast, it is challenging for adult mammals, including humans, to achieve regeneration (Takeo et al, 2015), and most adult wounds heal via repair, with a small amount of regeneration, depending on factors such as tissue type and the extent of injury.

Normal healing
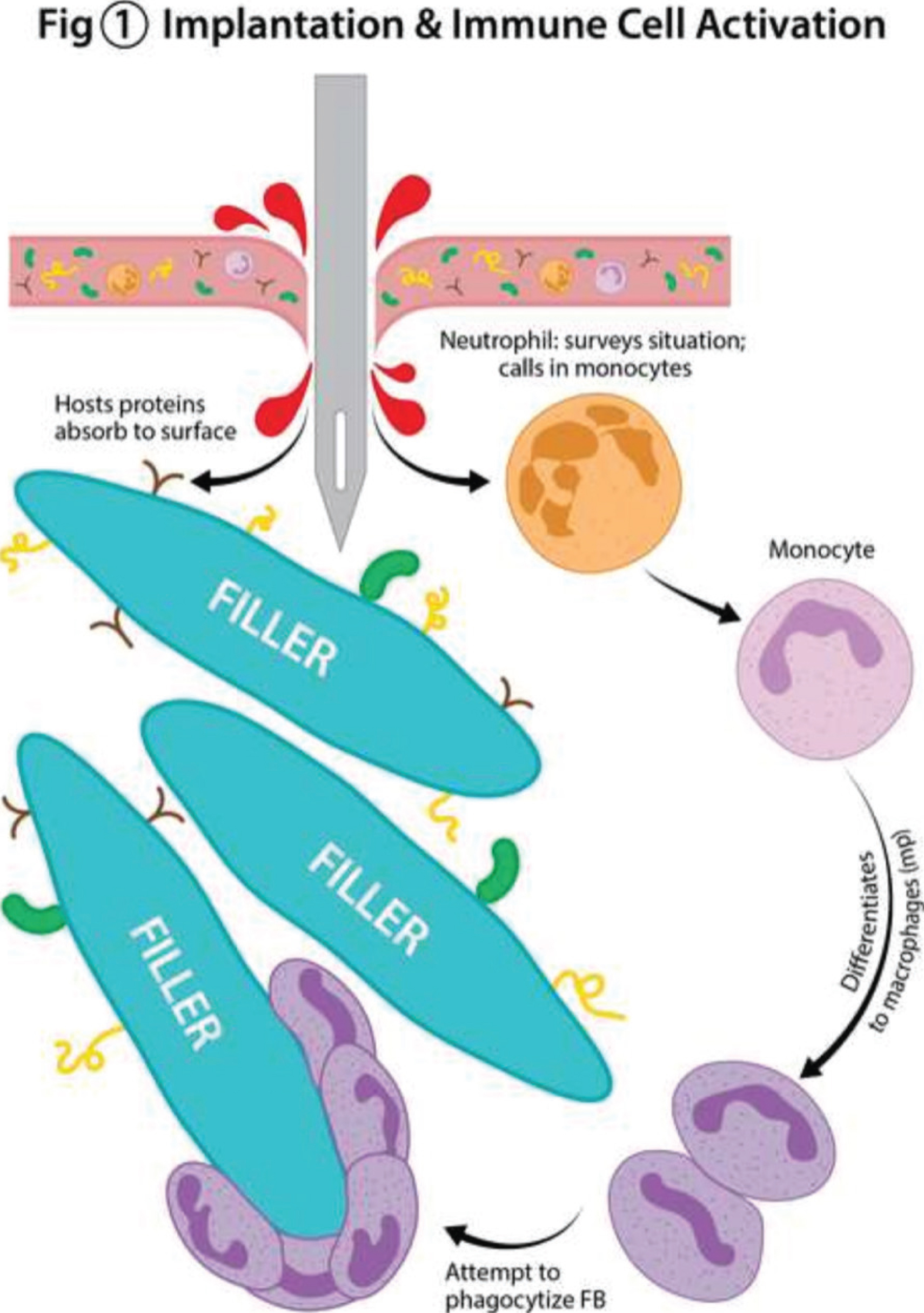
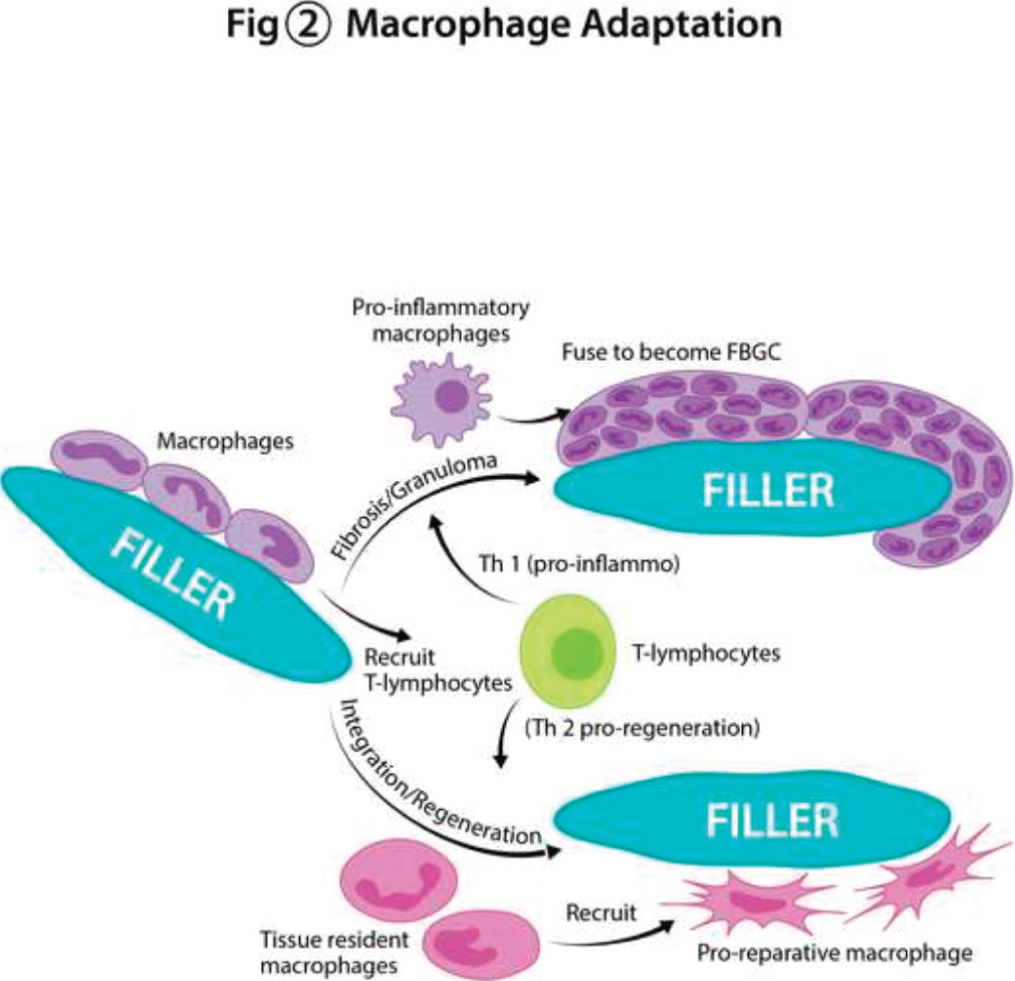
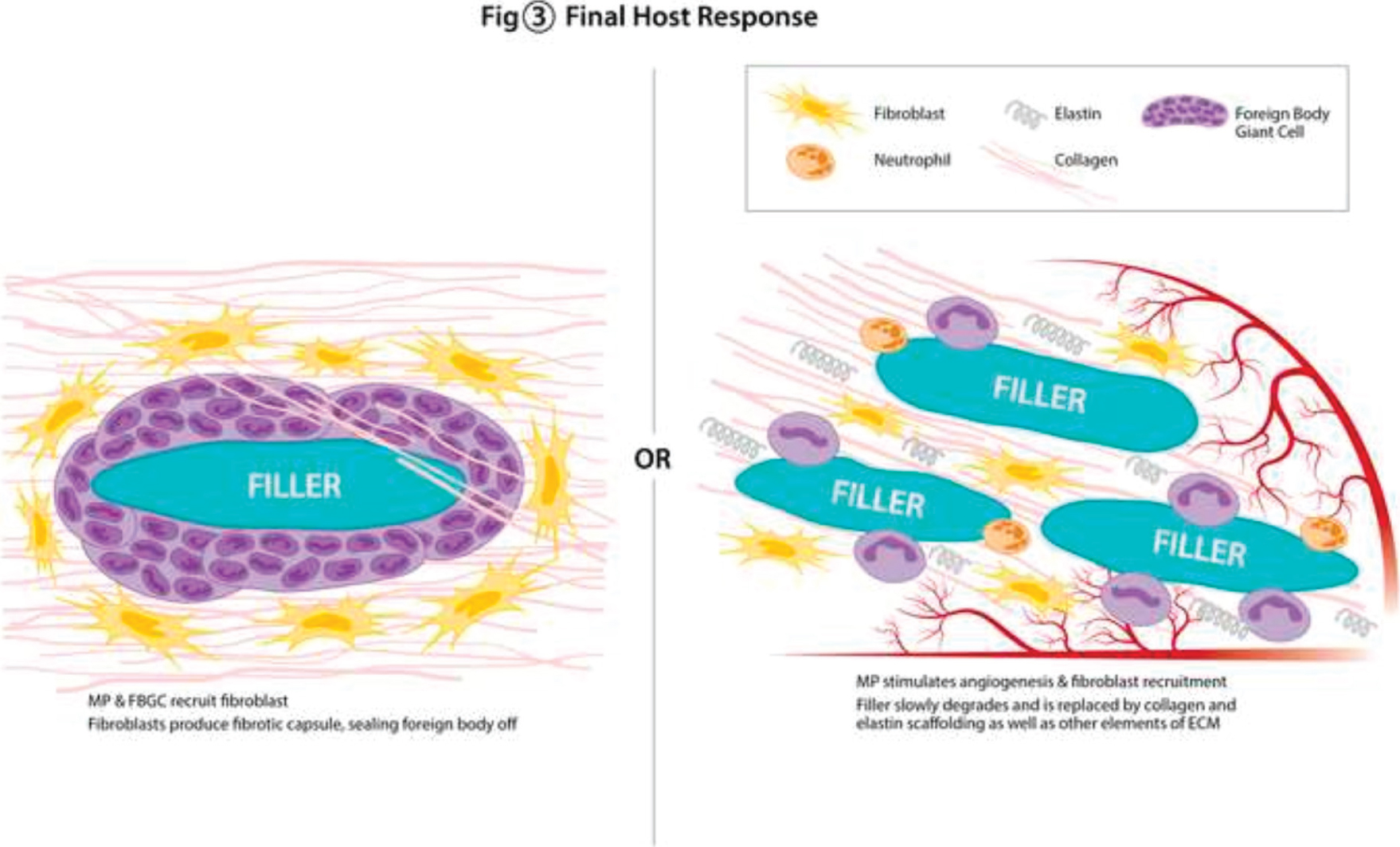
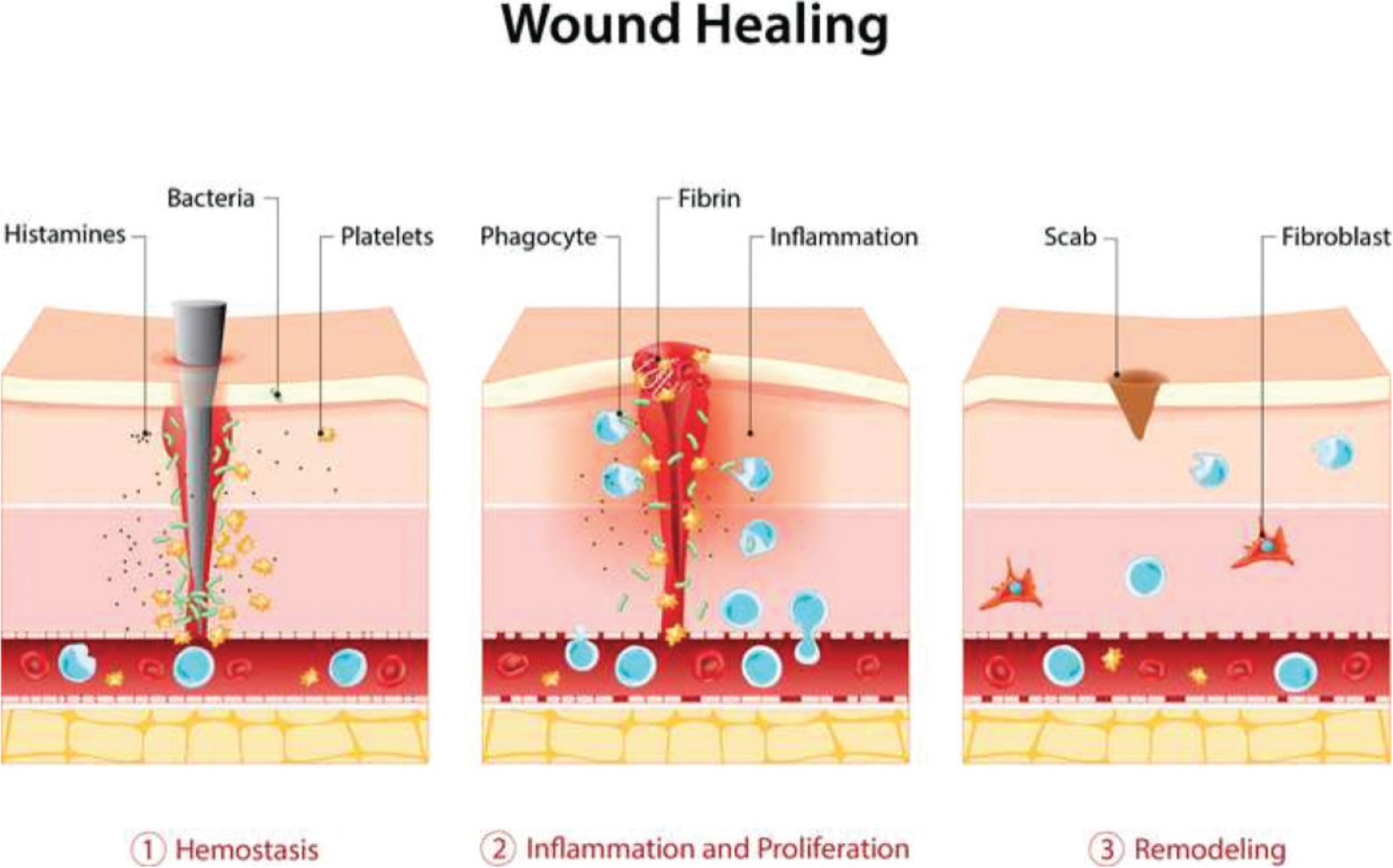
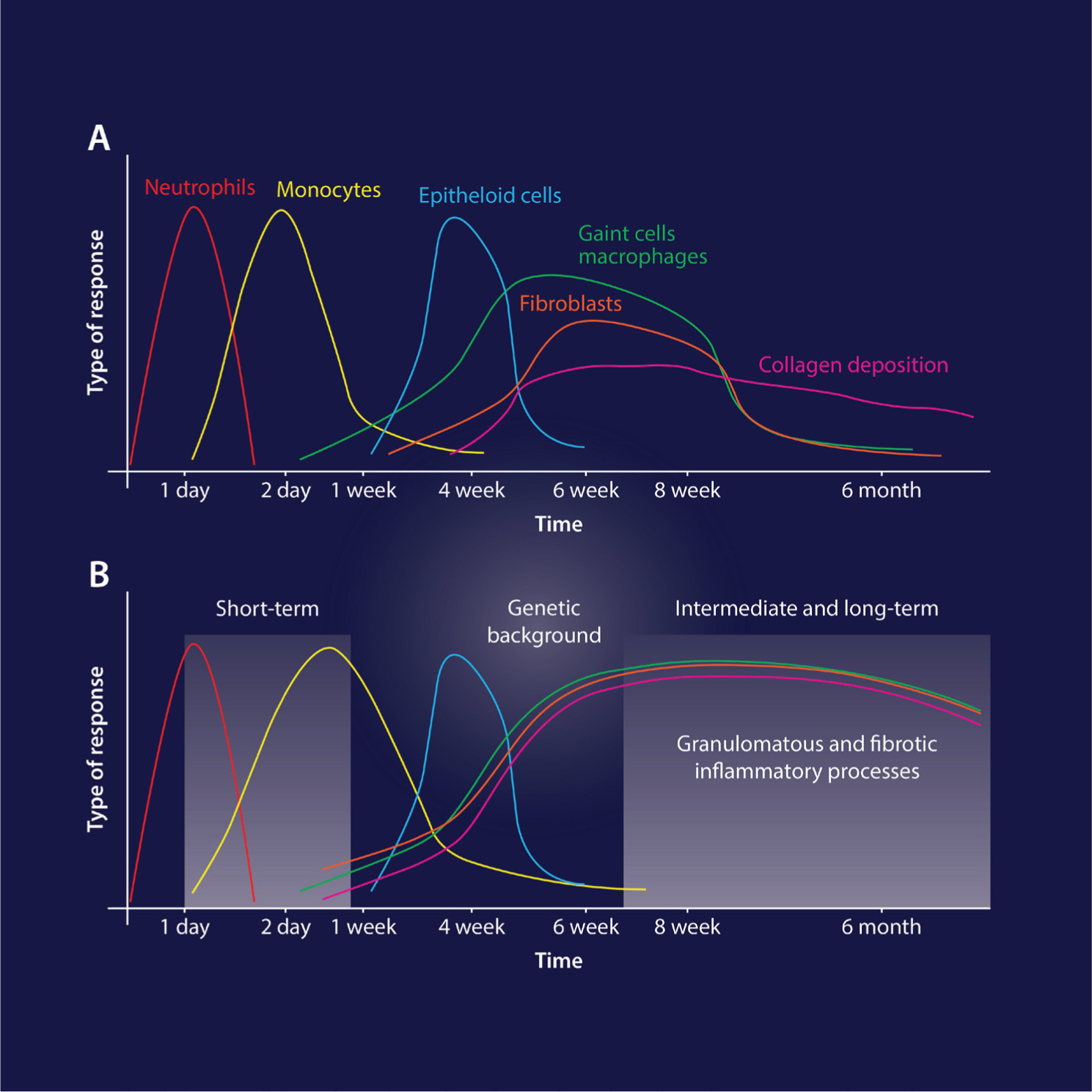
The normal wound healing cascade consists roughly of four phases: the hemostasis phase, inflammatory phase, the proliferative phase, and the maturational stage. The hemostasis and inflammatory stages are characterised by aggregation of platelets and neutrophils to the area, with subsequent release of growth factors, cytokines, and other chemical messengers to amplify the aggregation response. Recruited neutrophils begin debridement of devitalised tissue and phagocytosis of infectious agents (Eming et al, 2007) as well as foreign bodies (see the wound healing mechanisms in Figure 4). Monocytes arrive next on the scene; they can fuse to become multinucleated macrophages in order to phagocytise larger particles. Monocytes are excellent antigen presenters, activating T lymphocytes and preparing the immune system for further action. Macrophages secrete growth factors and other messengers, to regulate the change from the inflammatory phase, into the proliferative phase for reconstruction (Nicolau, 2005). Figures 1to3 portray the processes of implantation and immune cell activation, macrophage adaptation, and the final possible host responses respectively. Figure 4 illustrates the process of wound healing; and Figure 5 is a graph of host responses on a timeline.
» The creation of multiple micro injuries initiates the healing response, and the body is left to repair itself. This healing process is fascinating, complex, and still not completely elucidated. It encompasses two separate processes: regeneration and replacement «
In the case of injectable fillers, instead of a creating a large wound, a skin volumiser is injected. Conventional wisdom decrees that the presence of this filler then stimulates dermal fibroblasts to produce new collagen as well as other components of the extracellular matrix (ECM). This is often termed the biostimulatory effect of fillers. All the dermal fillers have the potential to act as biostimulators, coaxing fibroblasts to work harder. In a sense, this biostimulation leaves the skin better off, even after the product is absorbed, then if the product had never been injected in the first place. New collagen and other components of the ECM have been created and help improve skin quality.
Inflammatory response to filler injections?
Can this ‘stimulation’ be considered, then, essentially to be the initial inflammatory response of the wound healing cascade? Implantation of a foreign body into a host invariably prompts a wound healing response. In fact, inflammation around an implant particle is normal (Alijotas-Reig et al 2013). This inflammation occurs even though there may not be a true, devastating wound resulting in nonviable tissue. Bachour et al report that ‘all filler agents used for soft tissue filling are thought to elicit some degree of granulomatous inflammatory reaction; to a certain degree this is considered to be part of the normal physiological response’ (Bachour et al 2021). All the dermal fillers, if initiating this inflammatory cascade, then have the potential of this inflammation process going awry, continuing longer than it should, and causing fibrosis. Fibrosis, by definition, is the thickening and scarring of connective tissue. Fibrosis is common with implantation of medical devices. The failure of effective phagocytosis of an implanted medical device leads to granuloma formation (Alijotas-Reig, Fernandez-Figueras, Puig, 2013) with continued presence of activated macrophages. This, in turn, leads to eventual failure of the implant. The term frustrated phagocytosis has been used to describe the process fibrous encapsulation of foreign bodies that are too large to be engulfed and phagocytised (Barone et al, 2022). Frustrated phagocytosis results in a mass or nodule that can be classified as a foreign body granuloma. These can occur with all injectable dermal fillers, even hyaluronic acid (HA) and collagen (Lemperle et al, 2009). See again Figures 1to3 for a detailed illustration of this process, adapted from Huyer et al (2020).
» What, then, prevents this initial inflammatory process, caused by dermal filler injection, from directing healing to the repair pathway, creating fibrosis and scar collagen? What directs it to the regeneration pathway, creating functional, healthy skin components? How can aesthetic practitioners help assure a regenerative process instead of a reparative process? Can a reparative, fibrotic response even be predicted and avoided? «
Since tissue function is not disturbed, ideally, during or after injection of filler, it should result in a regenerative healing response, despite its inflammatory initiation. Fibrosis should not occur. Under optimal conditions healthy, non-scar collagen would be generated, and the dermis would appear and act more youthful. Indeed, Carruthers et al. (2014) proposed that this is the mechanism of action of hyaluronic acid fillers. Instead of an initiating an inflammatory granulomatous reaction, the injection of HA induces a mechanical stretching of the dermis, which in turn, elongates dermal fibroblasts, activating them and their production of collagen (Carruthers et al, 2014 & Wang et al, 2007). In the past HAs were not considered biostimulatory, due to their shorter duration of action. However, neocollagenesis after HA implantation has been demonstrated by researchers such as Wang et al, potentially qualifying HA as biostimulatory, and not just volumising.
Late inflammatory reactions to filler
Unfortunately, judging by the sheer number of reports in the literature on adverse and/or delayed inflammatory responses to filler, regenerative response to filler implantation is not the rule. There are number of so called ‘late inflammatory reactions’ or LIRs. Sometimes granulomatous reactions occur, months to years after injection, with the possibility of palpable, and occasionally, visible nodules. Foreign body granulomas are one type of LIR and can be defined as a tumor consisting immune cells, mainly macrophages and multinucleated giant cells (Lee & Kin, 2014). Infectious etiologies and/or biofilms are thought to be another major cause of LIRS. Delayed hypersensitivity reactions, both type I and IV, are also implicated in the development of LIRS, however a recent study disputes this, finding that neither type of hypersensitivity reaction plays a role in LIRS, at least with HA fillers (Decates et al 2021a).
Systemic reactions have been documented as well, including something called ASIA, or ‘autoimmune/autoinflammatory syndrome induced by adjuvants’. This constellation of signs and symptoms was coined by Schoenfeld and Agmon-Levin in 2011 and is also called Schoenfeld syndrome (Schoenfeld, Agmon-Levine, 2011). It refers to a constellation of autoimmune phenomena that are induced following exposure to substances with adjuvant activity (Watad, Sharif, Shoenfeld, 2017). An adjuvant is defined as an immunological molecule that functions through potentiating an antigen specific immune response (Bomford, 1998) and includes biomaterials like HA and other dermal fillers. While adjuvants themselves do not mount an immune response, they aid in the production of a robust reaction against their inoculated antigens, and influence both the adaptive and innate arms of the immune system (Watad, Sharif, Schoenfeld, 2017). The tendency for an ASIA type of reaction to fillers probably has a genetic basis: this has been proposed and studied by Alijotas-Rieg et al (2018). They report a link between the human leukocyte antigen (HLA) class I and II genes that predispose to autoimmune diseases and susceptibility to adjuvant triggering of T and B immune activation leading to inflammatory, immune related, late onset adverse reactions to biomaterials (Bell & Kelso, 2021, Alijotas-Rieg et al, 2018).
Decates and his colleagues found that patients with certain subtypes of HLA (the combination of subtypes B*08 and DRB1*03) had a 4-fold increase in the odds of developing immune related adverse events related to the injection of dermal fillers (Decates et al, 2021b). See Figure 5 for a graph of normal immune response versus granulomatous foreign body response on a background of genetic predisposition, after Alijotas-Reig et al (2013).
Histological evaluation of LIRs
A histological study of delayed onset complications of various types of fillers (collagen, hyaluronic acid, polyacrylamide gel and silicone oil) was published in a pathology journal for the edification of dermal pathologists. The authors describe four main types of reactions in biopsies approximately a year out from initial injection. These include 1) granulomatous reaction (most common) in the form of either a foreign body granuloma or infectious granuloma, 2) dermal pseudocysts with chronic inflammation, 3) dermal fibrosis and 4) eosinophilic panniculitis, a dense eosinophilic infiltrate in the subcutis, with some extension into the fat lobules (El-Khalawany et al, 2015). Foreign body granulomas can be furthered classified into 3 subtypes: cystic, associated with biologic gels such as HA; edematous, associated with fluids such as silicone and sometimes particulate fillers, and sclerosing, usually associated with the particulate fillers such as PLLA, PMA and CaHa (Graivier et al, 2018). The particulate fillers do not have a higher incidence of FBG formation when compared to that of HAs, however their clinical appearance may be more pronounced (Graivier et al, 2018), which of course, correlates to greater dissatisfaction of patients. What, then, prevents this initial inflammatory process, caused by dermal filler injection, from directing healing to the repair pathway, creating fibrosis and scar collagen? What directs it to the regeneration pathway, creating functional, healthy skin components? How can aesthetic practitioners help assure a regenerative process instead of a reparative process? Can a reparative, fibrotic response even be predicted and avoided?
Factors influencing biostimulatory and regenerative outcome
The product, the injector and the host/patient are all contributing factors to the replacement versus regenerative outcome after dermal fillers. The most cited issue, often claimed by the product manufacturers to avoid scrutiny of their product, is injector error. The manufacturers especially like to blame the injector for non-sterile technique resulting in biofilms, as a reason for late onset granulomas. This author, as well as others (Lemperle, 2020) have noted this trend. Of course, less than sterile technique resulting in infectious granulomas or biofilms, or blousing too large a volume of product leading to frustrated phagocytosis, and injecting in the wrong location, can all contribute to poorer outcomes, especially LIRs. Good, sterile technique is a must to ensure best outcomes for the patient.
Patient factors probably contribute more to the outcome of aesthetic injectables than generally acknowledged. In the aesthetic patient population, poor nutritional status secondary to mental disorders such as anorexia, bulima, vigorexia and muscle dysmorphia (Contesini et al, 2013) is more common than in a general medical patient population. In a compromised nutritional state, the body may resort to the quicker, easier replacement type of healing. It is common knowledge that patients with chronic diseases, chronic stress and/or chronic sleep deprivation, and patients with nicotine, alcohol, or other drug addictions are poor wound healers. In the aesthetic population, patients tend to be healthy in general and providers may not think to consider nutritional status as prognosticator of treatment success. As mentioned earlier, genetic predisposition to an ASIA type syndrome or autoimmune inflammation in general, may be a contributor of LIRs. Testing for different HLA genotypes may be possible in the future (Alijotas-Rieg, et al, 2018) but its development and feasibility is yet to be determined. The more generalised question of whether to treat patients with any type of autoimmune disease, active or in remission, is still up for debate.
» … genetic predisposition to an ASIA type syndrome or autoimmune inflammation in general, may be a contributor of LIRs. Testing for different HLA genotypes may be possible in the future but its development and feasibility is yet to be determined. The more generalised question of whether to treat patients with any type of autoimmune disease, active or in remission, is still up for debate «
Product properties are the final major consideration when pondering the regenerative abilities of dermal filler treatments. In fact, according to researchers outside the aesthetic arena, ‘the impact of the biological scaffolds on the immune system is currently believed to be the primary factor responsible for the positive regenerative outcomes’ (Chung et al 2017). These researchers, in oncology and wound healing engineering, are dealing with ill patients. Their goal is regeneration despite suboptimal healing environments. Griffin and colleagues reported that generation of an adaptive immune response from a biomaterial is sufficient to induce cutaneous regenerative healing (Griffin et al, 2021). Marin and her colleagues in Italy state that the cellular and molecular events that decide implant success and tissue regeneration are played at the interface between the foreign body and host inflammation, determined by the innate and adaptive immune system responses (Marin et al, 2019). Researchers are also experimenting with addition of drugs or other modulators such as growth factors, cytokines, chemokines, extracellular vesicles, or stem cells (Julier et al 2017, Larouche et al, 2018) to the biomaterials themselves to further ensure regenerative healing.
Conceivably, in the future, there will be dermal fillers with these additives. The available evidence seems to point the biomaterial’s influence on the host’s adaptive and innate immune system as the most important factor in determining its regenerative healing capabilities. The ability of the injected product to induce a favourable, regenerative response, and avoid a fibrotic one, should be a major consideration in deciding which product to use. Yet, the product manufacturers of the specific dermal fillers do not attempt to differentiate themselves on these grounds. In this author’s opinion, regenerative abilities of the filler should be one of its most important traits! Of the fillers available on the market, some are demonstrably better than others at regenerative healing. HA, Poly-L-Lactic Acid and Calcium Hydroxylapatite all have biostimulative abilities. Many injectors prefer hyaluronic acid products because of their ease of dispersal with hyaluronidase in the event of an undesired outcome or serious problem such as vascular occlusion. Many also like it because it is ‘natural’ and already found in the ECM. In fact, hydrogels, (HA is a type of hydrogel) have been used in regenerative applications for many decades because of their biocompatibility and similarity in structure to the native extracellular matrix (Dimatteo, Darling & Segura, 2018). As a natural skin component, HA has favorable effects on the fibroblast phenotype in vitro and in vivo, including high cell proliferation and collagen synthesis (Cabral et al, 2020).
» The available evidence seems to point the biomaterial’s influence on the host’s adaptive and innate immune system as the most important factor in determining its regenerative healing capabilities. The ability of the injected product to induce a favourable, regenerative response, and avoid a fibrotic one, should be a major consideration in deciding which product to use. Yet, the product manufacturers of the specific dermal fillers do not attempt to differentiate themselves on these grounds «
However, not all HAs are created equal. In an effort to delay absorption and increase longevity of action, HAs have been manipulated in the laboratory to have different degrees of crosslinking, different particle sizes and different concentrations. These different HAs are associated with differing rates of LIRs (Artzi et al, 2020). More concentrated products with greater degrees of crosslinking have longer duration of effect, but they also increase reactivity in the body and thus the risk of inflammation and granuloma formation (Funt & Pavicic, 2013). Choi et aI. (2021) also found that with increasing the crosslinking in HA products, there was an increased inflammatory response in the host. In other words, the more manipulated the HA molecule is, the more likely it is to be viewed by the immune system as a foreign body and engender a fibrotic response instead of a regenerative one. In truth, HAs, especially high G’ HAs, may not be the benign, free-of-long-term complications, safe fillers they are touted to be. Poly-L-Lactic Acid and Calcium Hydroxyapatite fillers are often lumped together as THE biostimulatory fillers, because of their duration of action and proven ability to generate collogen synthesis. When examined closely, however, the mechanism of this collagen neogenesis is quite different. Poly-L-Lactic Acid or PLLA is a synthetic, biocompatible, and biodegradable polymer of lactic acid that has been used safely in various medical applications for more than three decades (Vleggaar, 2005; Breithaupt & Fitzgerald, 2015). However, the true mechanism of action begins with a subclinical inflammatory tissue response after implantation, followed by encapsulation of the particles and subsequent fibroplasia (Breithaupt & Fitzgerald, 2015). Other authors have described it as ‘an intense inflammatory reaction to a foreign body, represented by innumerous multinucleated cells, surrounded by a fibrous capsule’ (Cabral et al, 2020). In a study specifically designed to elucidate the mechanism of action of PLLA, Stein et al reports that the biological mechanism generating the desired augmenting effect of PLLA is most likely mediated by macrophages and FBGC (foreign body giant cells) that recognise PLLA as a foreign body (Stein et al, 2015). Essentially, a foreign body response with resulting fibrosis is responsible for the eventual volumetric improvement from PLLA. This could not be considered regenerative. Calcium Hydroxyapatite, in comparison, may be more regenerative. Injectable CaHa consists of 30% microspheres, approximately 25-45 um in diameter, suspended in a 70% sodium carboxymethylcellulose/glycerin/sterile water gel. Once injected the CMC gel gradually dissipates leaving the microspheres at the injection point where they induce neocollagenesis by fibroblast activation (Loghem, Yutskovskaya, Werschler, 2015). Too large to be directly phagocytised but too small to elicit significant FBGC formation, it is thought that microspheres are degraded by acids released by macrophages to slowly dissolve the CaHa into its substrates of calcium and phosphate ions (Loghem ed. 2021) which are then eliminated by the kidneys. Canine studies have demonstrated that supraperiosteal implantation of CaHa particles into soft tissue resulted in increased connective tissue around the microspheres without significant inflammation (Emer, Sundaram, 2013) and no capsule formation was seen in any of the specimens obtained (Coleman et al, 2008). Couderot and colleagues noticed that in addition to fibroblast proliferation, CaHa also improved contractile function, and brought wrinkle fibroblasts (WF) contractile functions back to the level of normal aged fibroblasts (NF) (Couderot et al, 2016; Trindade de Almedianet al, 2019). Additionally, an MRI study performed by Dr. Tatjana Pavicic after CaHa injection for malar enhancement demonstrated intermediate MRI signal intensity immediately after injection. Reimaging two and a half years later revealed no visible CaHa but tissue volume remained increased, indicating a collagen stimulating effect (Pavicic, 2015). In a recent study determining an optimal dilution ratio for CaHa, it was discovered that direct contact with fibroblasts is a key factor in inducing neocollagenesis (Nowag et al, 2022). Though it is not clear the exact mechanism for this, fibroblast mechanoreceptors are thought to play a role (Nowag et al, 2022). Thus, CaHa may behave similarly to HAs in production of collagen by stretching or pressurising the fibroblasts, not inducing a foreign body inflammatory response. The benefit of CaHa is its longer duration of action and its breakdown into non inflammatory by-products.

Longer term fillers such as polycaprolactone and polymethymethacrylate, as well as permanent fillers such as medical grade silicone, have interesting stories regarding regenerative capabilities, but those stories are beyond the scope of this paper. More research is needed on all types of fillers and the immune response they illicit, as well as ways to possibly manipulate this immune response to favor a regenerative pathway. The little axolotl may harbour secrets to this end that can be used for the benefit of all patients, not just aesthetic ones. The choices of dermal fillers are many, with more coming to market every year. An aesthetic injector must be aware not only of the rheologic properties of their fillers of choice but also of the histologic response provoked by these fillers in their patients. The goal of aesthetic medicine is better-looking patients; the goal of aesthetic regenerative medicine is better-looking patients with healthier skin and bodies. There is a subtle shift happening in the aesthetic world, with savvy patients requesting a more regenerative approach to their treatments. Providers in the future will need to understand these concepts and be able to provide truly regenerative treatments.
» The goal of aesthetic medicine is better-looking patients; the goal of aesthetic regenerative medicine is better-looking patients with healthier skin and bodies. There is a subtle shift happening in the aesthetic world, with savvy patients requesting a more regenerative approach to their treatments «
Key points
- Regeneration refers to a type of healing in which new growth completely restores portions of damaged tissue to their normal state, whereas replacement refers to healing of severely damaged tissues by laying down connective tissue, commonly called scarring (Krafts, 2010), with less function or nonfunction of the new tissue
- The goal of regenerative medicine is to provide a substitute for tissues lost to trauma, disease, congenital abnormalities (Chung et al, 2017) and to restore tissue function back to physiological activity (Griffin et al, 2021)
- Not all HAs are created equal. In an effort to delay absorption and increase longevity of action, HAs have been manipulated in the laboratory to have different degrees of crosslinking, different particle sizes and different concentrations
- The goal of aesthetic medicine is better-looking patients; the goal of aesthetic regenerative medicine is better-looking patients with healthier skin and bodies
CPD reflective questions
- This article explores the mechanisms of biostimulation and wound healing. How would you apply the knowledge from this article to your professional practice?
- ‘In the aesthetic population, patients tend to be healthy in general and providers may not think to consider nutritional status as prognosticator of treatment success’. To what extent would this apply to your current practice?
- How can aesthetic practitioners help assure a regenerative process instead of a reparative one?